





Conditions, Investigations and Treatments
There is an increasingly complex mix of abdominal wall hernias diagnosed in an increasingly diverse population group. To cater to this there is a plethora of rapidly expanding surgical products being used in hernia surgery. Similarly, there is also a fast-evolving number of surgical techniques being employed in hernia repairs.
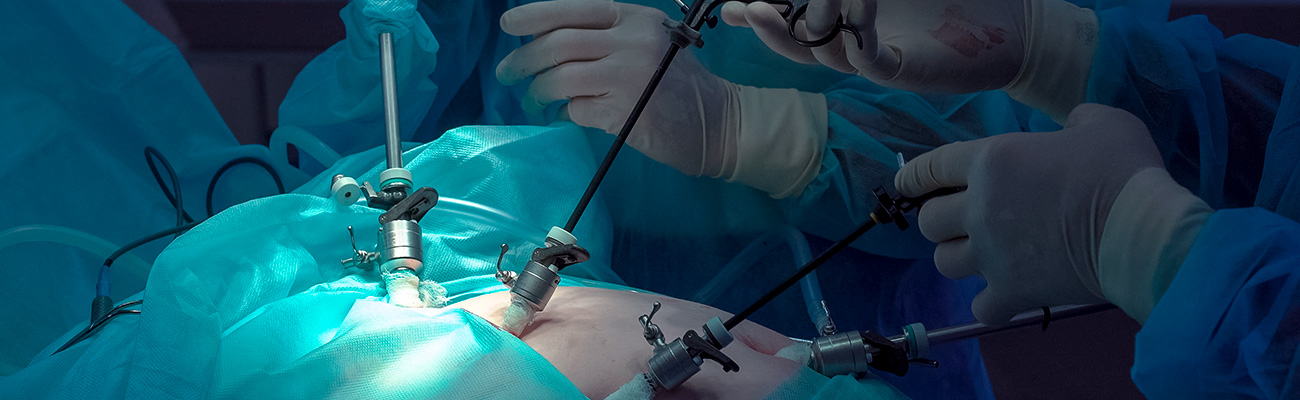
We offer a service from diagnosis, assessment and definitive management of multiple surgical diseases that include both traditional open surgery and the latest minimally invasive advanced laparoscopic (keyhole) and endoscopic techniques.
Products used in hernia repair
Hernias – overview
Hernias occur when there is a weakness in the abdominal musculature allowing the abdominal contents to push through.
The common abdominal organs involved in hernia are the omentum (fat in the abdominal cavity) and the small bowel. However, any organ within the abdominal cavity can be involved in the hernia. A hernia can be aggravated by coughing and straining associated with constipation or heavy lifting.
The common abdominal organs involved in hernia are the omentum (fat in the abdominal cavity) and the small bowel. However, any organ within the abdominal cavity can be involved in the hernia. A hernia can be aggravated by coughing and straining associated with constipation or heavy lifting.

Types of hernia.

Hernia locations.
The commonest site for hernia is the groin (inguinal or femoral hernia).
Other hernia sites include the navel (umbilical hernia), in the midline of the upper abdomen (epigastric hernia) and at the site of a previous operation (incisional hernia).
Other hernia sites include the navel (umbilical hernia), in the midline of the upper abdomen (epigastric hernia) and at the site of a previous operation (incisional hernia).

Incisional hernia.
Symptoms
Presentation of abdominal wall hernias:
Hernia typically presents with a noted bulge under the skin.
The bulge is commonly associated with pain or discomfort, especially with physical activities.
There may be associated/referral pain, depending on the hernia site. For example, with the groin hernia, there may be associated testicular ache/discomfort.
Initially, the hernia can be pushed back into the abdomen (reducible hernia). Similarly, the bulge will reduce in size or disappear when the patient lies down.
Hernia typically presents with a noted bulge under the skin.
The bulge is commonly associated with pain or discomfort, especially with physical activities.
There may be associated/referral pain, depending on the hernia site. For example, with the groin hernia, there may be associated testicular ache/discomfort.
Initially, the hernia can be pushed back into the abdomen (reducible hernia). Similarly, the bulge will reduce in size or disappear when the patient lies down.
Natural history of hernia
A hernia will not disappear on its own accord. With time, hernia tends to increase in size and become more symptomatic.
It may become very difficult or impossible to push back into the abdomen (irreducible/incarcerated hernia).
It may become very difficult or impossible to push back into the abdomen (irreducible/incarcerated hernia).
Occasionally, the blood supply to the hernia content of the hernia can be compromised, causing the hernia content to die (strangulated hernia), which is a true surgical emergency.

Strangulated hernia.
The symptoms of strangulated hernia are:
The patient must seek immediate medical assistance should this occur.
- Sudden appearance of a lump or sudden increase in size of a pre-existing lump.
- The lump is very tender to touch.
- The lump will not be able to be pushed back into the abdomen.
- Severe pain associated with the lump.
- There may be associated nausea, vomiting or abdominal bloating/distention.
The patient must seek immediate medical assistance should this occur.
Hernia repair
Hernias usually are repaired at the patients’ convenience.
Important facts in making the decision are:
Hernia repair is performed by the open technique or using the laparoscopic (key-hole surgery) methods. In both methods, the hernia content is pushed/pulled back into the abdomen. The hernia defect is then sutured closed and covered with a mesh to minimise recurrence.
The mesh is a synthetic material that will be incorporated into the body with time, giving strength to the repair. It is very inert and thus is not rejected by the body. The mesh is not noticeable or felt in the body. The use of mesh has reduced the hernia recurrence rate from 5–10% to less than 3% for groin hernia and less than 5% for other types of hernias.
Important facts in making the decision are:
- The hernia will never improve or heal by itself.
- On most patients, the hernia and its symptoms will get worse with time. Certain physical activities (work and recreational) can make this progression occur at a faster rate.
- Until the hernia is repaired, there is a risk of strangulation (see above). The occurrence of this situation is unpredictable. Should it occur the patient would require emergency surgery within a few hours, to avoid clinically significant mortality and morbidity to the patient. For this reason, an increasing number of employers will not allow any employee with a known hernia to return to work, if the employee works in remote areas (such as in the mining sector).
Hernia repair is performed by the open technique or using the laparoscopic (key-hole surgery) methods. In both methods, the hernia content is pushed/pulled back into the abdomen. The hernia defect is then sutured closed and covered with a mesh to minimise recurrence.
The mesh is a synthetic material that will be incorporated into the body with time, giving strength to the repair. It is very inert and thus is not rejected by the body. The mesh is not noticeable or felt in the body. The use of mesh has reduced the hernia recurrence rate from 5–10% to less than 3% for groin hernia and less than 5% for other types of hernias.

Types of mesh.

Types of mesh.
See more about Mesh here.
Types of hernia repairs
Open hernia repair
The open hernia repair technique requires a single incision (cut) on the abdominal wall. The abdominal muscle layer is cut and separated to reveal the hernia. This is then replaced into (‘reduced’) into the abdominal cavity.
The hernia defect is then sutured closed. Typically, a mesh is placed to reinforce the repair. The muscle layers and skin are then sutured closed.
Laparoscopic hernia repair
The laparoscopic (‘key hole’) is done through a number of incisions through the skin and anterior abdominal wall muscle. Each of these incisions is typically a lot smaller than the incision for open surgery. The abdominal cavity is then expanded with carbon dioxide gas.
The hernia is identified and reduced (pulled back into the abdominal cavity).
The open hernia repair technique requires a single incision (cut) on the abdominal wall. The abdominal muscle layer is cut and separated to reveal the hernia. This is then replaced into (‘reduced’) into the abdominal cavity.
The hernia defect is then sutured closed. Typically, a mesh is placed to reinforce the repair. The muscle layers and skin are then sutured closed.
Laparoscopic hernia repair
The laparoscopic (‘key hole’) is done through a number of incisions through the skin and anterior abdominal wall muscle. Each of these incisions is typically a lot smaller than the incision for open surgery. The abdominal cavity is then expanded with carbon dioxide gas.
The hernia is identified and reduced (pulled back into the abdominal cavity).
The hernia defect is closed with sutures and a mesh is placed covering the sutured defect. The mesh is held in placed with the use of anchoring sutures and plastic staples.

Laparoscopic inguinal hernia mesh.
Complications
Each approach has its own advantages and disadvantages, which will be discussed in detail at your consultation session. The greatest risk of undergoing hernia repair is that the hernia can come back (recurrence).
Fortunately, the recurrence rate is low with modern surgical techniques performed by experienced dedicated hernia surgeons.
Fortunately, the recurrence rate is low with modern surgical techniques performed by experienced dedicated hernia surgeons.
Postoperative care
Discharge
Upon discharge, patients will be provided with a script for analgesia and any relevant medications. Information about the medication will also be provided.
We will also provide information on a recommended regime for the analgesia. This includes a table of the regime. Patients will be educated on the use of this during their inpatient stay and are strongly encouraged to continue using it upon discharge. (It will be given to you at initial consultation with other relevant information. Please take the time to read all the information before the surgery date).
My Post Operative Care Consultant will contact patients a few days after discharge to ensure the recovery occurs smoothly. Any concern will be addressed.
A post-operative appointment will then be made.
We will also provide information on a recommended regime for the analgesia. This includes a table of the regime. Patients will be educated on the use of this during their inpatient stay and are strongly encouraged to continue using it upon discharge. (It will be given to you at initial consultation with other relevant information. Please take the time to read all the information before the surgery date).
My Post Operative Care Consultant will contact patients a few days after discharge to ensure the recovery occurs smoothly. Any concern will be addressed.
A post-operative appointment will then be made.
Post-operative
Most patients will require two weeks off work. This is to enable more comfortable recovery. Patients may require strong painkillers to help them through this period. These medications may cause some sedative effect on some patients.
Activities and restrictions after surgery vary according to the location of the hernia, size and complexity of the hernia and the repair method. Most patients are restricted to no lifting for 2 weeks and then a lifting limit of 5–10 kgs and to limited physical activity. These limits can vary for up to 3–4 weeks for laparoscopic inguinal surgery, to 6 to 8 weeks for ventral and incisional hernias. Patients recovering from very large ventral or incisional hernias may need to make a permanent life-style change to reduce the chance of recurrence.
Most patients will be able to drive after two weeks. This will depend on patients’ comfort level, the drugs that are being taken and ability to safely handle the car.
Activities and restrictions after surgery vary according to the location of the hernia, size and complexity of the hernia and the repair method. Most patients are restricted to no lifting for 2 weeks and then a lifting limit of 5–10 kgs and to limited physical activity. These limits can vary for up to 3–4 weeks for laparoscopic inguinal surgery, to 6 to 8 weeks for ventral and incisional hernias. Patients recovering from very large ventral or incisional hernias may need to make a permanent life-style change to reduce the chance of recurrence.
Most patients will be able to drive after two weeks. This will depend on patients’ comfort level, the drugs that are being taken and ability to safely handle the car.
See more about:
Clinical Associate Professor Hairul Ahmad
MB BS, FACEM (1999), FRACS, MS
Suite 12, Waikiki Specialist Centre,
217 Willmott Drive, Waikiki
Practice Details
Waikiki
Suite 12, Waikiki Specialist Centre,
217 Willmott Drive, Waikiki WA 6169
(08) 9592 2298
Fax: (08) 6314 1524
or email us
Office hours
9am–4pm Monday to Thursday
Affiliations




© 2024 All Rights Reserved. Content and images on this website are subject to copyright.
Email us | Sitemap | Disclaimer | Login