





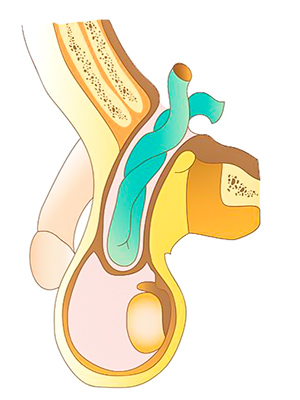
Inguinal Hernia
There are two types of inguinal hernias – direct and indirect inguinal hernias.
This classification is dependent on where the hernia defect is.
This classification is dependent on where the hernia defect is.

Inguinal hernia.

Symptoms
Both types of inguinal hernias present:
- As a lump in the groin. This can present suddenly or gradually. Initially this lump will disappear with lying down or gentle pressure (reducible hernia) but may progress to a lump that will be permanently present (irreducible hernia)
- with pain or discomfort in the groin area
- and a ache in the testicle.
Risk factors
- males are more than likely than female to develop inguinal hernias
- certain medical conditions, such as: chronic cough, chronic liver disease, or chronic lung disease
- excess weight
- pregnancy
- past history of one hernia.
Clinical types of inguinal hernia
Reducible hernias
These are hernias with lumps that ‘disappear’ on lying down and the lump can easily be ‘pushed back’.
Irreducible hernias
In these hernias, the lumps no longer disappear on lying down and are not able to completely be ‘pushed back’.
Strangulated hernia
This is a true surgical emergency. Patient must seek medical assistance immediately.
This occurs when the hernia content is being deprived of its blood supply. Without immediate surgical correction, the hernia content will die. This is especially critical if bowel is part of the hernia content. This can carry significant mortality for the patient.
Symptoms/signs of a strangulated hernia:
These are hernias with lumps that ‘disappear’ on lying down and the lump can easily be ‘pushed back’.
Irreducible hernias
In these hernias, the lumps no longer disappear on lying down and are not able to completely be ‘pushed back’.
Strangulated hernia
This is a true surgical emergency. Patient must seek medical assistance immediately.
This occurs when the hernia content is being deprived of its blood supply. Without immediate surgical correction, the hernia content will die. This is especially critical if bowel is part of the hernia content. This can carry significant mortality for the patient.
Symptoms/signs of a strangulated hernia:
- Sudden appearance of a lump.
- The lump is very painful and tender to touch.
- There may be associated nausea, vomiting and abdominal distention/bloating.
- The overlying skin may be swollen, slightly reddish discolouration and hot to the touch.
Repair of inguinal hernias
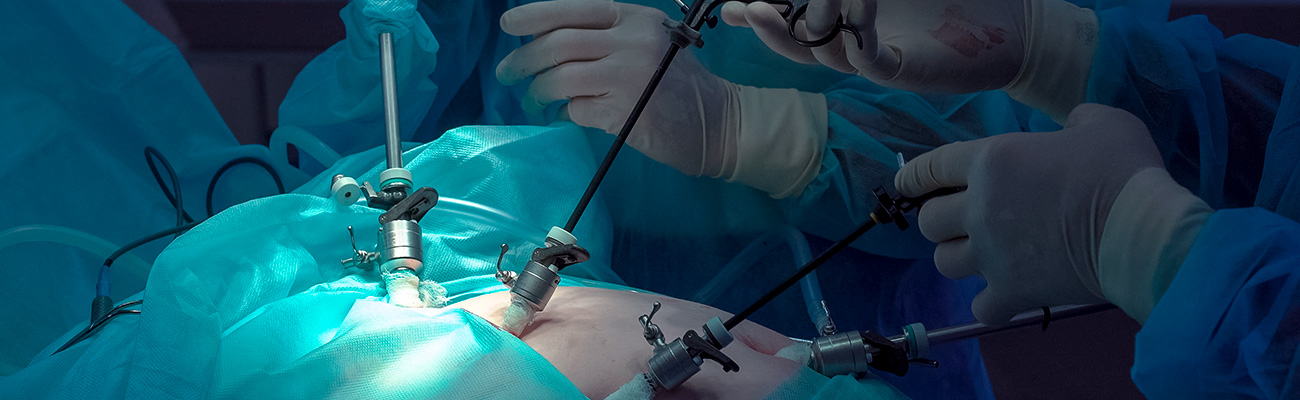
Inguinal hernias may be repaired through an open (traditional) repair or through laparoscopic (keyhole) repair.
Open Inguinal Hernia Repair
An incision is made over the groin. The most superficial of the abdominal muscles is then split and the hernia sac is identified. This is freed from the blood vessels, spermatic cord to the testicle (in males) or round ligament (in females). The hernia is then reduced.

Normal groin anatomy.

Hernia (operative photo).
A mesh repair is performed by placing a piece of mesh either between the muscle layers or deep to the muscle. The overlying muscle and skin are then closed with sutures.

Mesh placed in inguinal hernia repair.
Potential complications of the repair (0–5%):
- Haematoma (bruising). This can occur not only at the incision site but also in the scrotum (in the male). This will settle with time. It rarely requires intervention.
- Wound infection (< 1%).
- Recurrence of the hernia (≈ 2% with the use of mesh).
- Persisting local pain (1–2%).
- Damage to the testicular blood supply. This is very rare. The risk is higher in surgery for recurrence hernia. However if it does occur, it will result in shrinkage of the testicle. Ability to have children is normal provided there is a normal functioning testicle on the other side.
Laparoscopic repair ('keyhole surgery')
This can be done through the intraperitoneal (‘inside the abdomen’) or the extraperitoneal (‘outside of the abdomen’).
The peritoneum is a ‘sac’ in the inside of the muscle layers of the abdomen, which contains all the abdominal organs. The intraperitoneal space is the space within the sac. The extraperitoneal space is the space between the peritoneal sac and overlying muscle layer.
The peritoneum is a ‘sac’ in the inside of the muscle layers of the abdomen, which contains all the abdominal organs. The intraperitoneal space is the space within the sac. The extraperitoneal space is the space between the peritoneal sac and overlying muscle layer.
This surgical approach may not be possible if a patient has had surgery in the lower abdomen due to the scarring of tissue resulting from the previous surgery.

The intraperitoneal space.
Laparoscopic Totally Extraperitoneal (TEPP) Inguinal hernia repair
This procedure tends to be reserved for patients with bilateral hernias (hernias in both side of the groin) or patients who have had previous open hernia surgery. However it is also increasingly being employed for a single-sided groin hernia.
This is performed through three small incisions in the abdominal wall. An incision (≈ 2 cm) is made to the side of the umbilicus, which is deepened through the abdominal muscle (the ‘six pack’ muscle). The space behind the abdominal muscle wall (the extraperitoneal space) is then developed with the use of special surgical balloons and then blowing carbon dioxide into the space. Two 5mm incisions are then made in the anterior abdominal wall, between the umbilicus and the pelvic bones. The laparoscope is inserted to view the area and identify the hernia.
This is performed through three small incisions in the abdominal wall. An incision (≈ 2 cm) is made to the side of the umbilicus, which is deepened through the abdominal muscle (the ‘six pack’ muscle). The space behind the abdominal muscle wall (the extraperitoneal space) is then developed with the use of special surgical balloons and then blowing carbon dioxide into the space. Two 5mm incisions are then made in the anterior abdominal wall, between the umbilicus and the pelvic bones. The laparoscope is inserted to view the area and identify the hernia.

The hernia is then reduced (“pulled back to its normal anatomical location”). A mesh is then placed to cover the hernia defect. The carbon dioxide is then removed from the operating space. The incisions are closed with sutures.
Note: An operative DVD of this procedure will be shown during your consultation.
Note: An operative DVD of this procedure will be shown during your consultation.
Laparoscopic Transabdominal PrePeritoneal (TAPP) inguinal hernia repair
This is a “keyhole” (laparoscopic) approach. However, the repair is done within the intraperitoneal cavity (see diagram above).
Three small incisions are made on the abdominal wall, through which the procedure is performed. The hernia defect is identified and the hernia ‘reduced’ (hernia content pulled back into the abdominal cavity). The peritoneum lining is then incised and reflected away from the overlying muscular layer. The hernia defect is closed with suture. A mesh is placed covering the hernia defect. The peritoneal layer is then restored to normality.
The skin incisions are closed with dissolvable sutures.
Three small incisions are made on the abdominal wall, through which the procedure is performed. The hernia defect is identified and the hernia ‘reduced’ (hernia content pulled back into the abdominal cavity). The peritoneum lining is then incised and reflected away from the overlying muscular layer. The hernia defect is closed with suture. A mesh is placed covering the hernia defect. The peritoneal layer is then restored to normality.
The skin incisions are closed with dissolvable sutures.
Complications
Each approach has its own advantages and disadvantages, which will be discussed in detail at your consultation session. The greatest risk of undergoing hernia repair is that the hernia can come back (recurrence).
Fortunately, the recurrence rate is low with modern surgical techniques performed by experienced dedicated hernia surgeons.
Complications specific to laparoscopic repair
Injury to intestine, bladder, and major blood vessels.
This will require immediate repair. If possible this will be performed laparoscopically (keyhole), however it is possible that an open (bigger) incision may be required.
Gas embolism (gas bubble entering into the blood stream). This is very rare, but if it occurs it can be fatal.
Other potential complications:
Fortunately, the recurrence rate is low with modern surgical techniques performed by experienced dedicated hernia surgeons.
Complications specific to laparoscopic repair
Injury to intestine, bladder, and major blood vessels.
This will require immediate repair. If possible this will be performed laparoscopically (keyhole), however it is possible that an open (bigger) incision may be required.
Gas embolism (gas bubble entering into the blood stream). This is very rare, but if it occurs it can be fatal.
Other potential complications:
- Haematoma (bruising). This can occur not only at the incision site but also in the scrotum (in the male). This will settle with time. It rarely requires intervention.
- Wound infection (< 1%).
- Recurrence of the hernia (≈ 2% with the use of mesh).
- Persisting local pain (1–2%).
- Damage to the testicular blood supply. This is very rare. The risk is higher in surgery for recurrence hernia. However, if it does occur, it will result in shrinkage of the testicle. The ability to have children is normal provided there is a normal functioning testicle on the other side.
Postoperative care
Post Discharge
Most patients will only need to stay overnight after the procedure.
For details see: What happens after my discharge from hospital?
For details see: What happens after my discharge from hospital?
Post-operative recovery
Patients are strongly advised to take 2 weeks off work, when appropriate. Patients are also advised that they should not do any heavy lifting for about a month postoperatively.
Please see: What happens after my Surgery?
Please also see: Hernia – overview
Please see: What happens after my Surgery?
Please also see: Hernia – overview
Clinical Associate Professor Hairul Ahmad
MB BS, FACEM (1999), FRACS, MS
Suite 12, Waikiki Specialist Centre,
217 Willmott Drive, Waikiki
Practice Details
Waikiki
Suite 12, Waikiki Specialist Centre,
217 Willmott Drive, Waikiki WA 6169
(08) 9592 2298
Fax: (08) 6314 1524
or email us
Office hours
9am–4pm Monday to Thursday
Affiliations




© 2024 All Rights Reserved. Content and images on this website are subject to copyright.
Email us | Sitemap | Disclaimer | Login