





Umbilical and epigastric hernia
Both umbilical and epigastric hernias can typically also be labelled as ventral hernias.
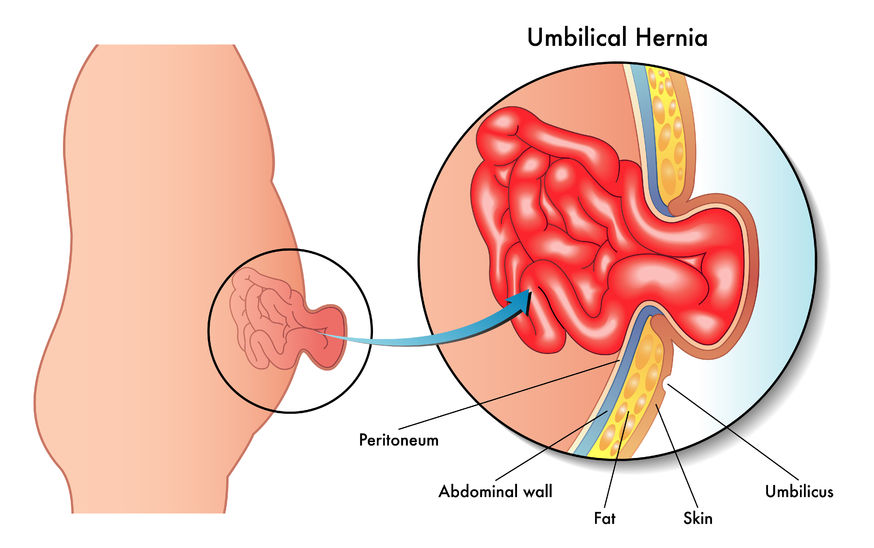
An umbilical hernia presents as a lump in the belly button with associated pain or discomfort.
Similarly a ventral hernia presents as a lump protruding through the abdominal wall between the belly button and the rib margins. It normally contains fat. However large hernia may contain other abdominal organs such as small bowel or stomach.
It may also be associated with recti diastasis (please see: recti diastasis).
For general information on hernias, please see: Hernia – overview
An umbilical hernia presents as a lump in the belly button with associated pain or discomfort.
Similarly a ventral hernia presents as a lump protruding through the abdominal wall between the belly button and the rib margins. It normally contains fat. However large hernia may contain other abdominal organs such as small bowel or stomach.
It may also be associated with recti diastasis (please see: recti diastasis).
For general information on hernias, please see: Hernia – overview
Repair of umbilical and epigastric hernias
Umbilical and epigastric hernias may be repaired through an open (traditional) method or by laparoscopic (keyhole) technique.
The choice of which technique to be employed for the repair will be discussed thoroughly at your consultation session. The factors taken into consideration are:
The choice of which technique to be employed for the repair will be discussed thoroughly at your consultation session. The factors taken into consideration are:
- the size of the hernia
- the number of hernias
- whether there is any associated recti diastasis (please see: recti diastasis)
- possible complications of each technique
- patient choice.
Open umbilical/epigastric repair
This approach is used to repair small umbilical hernia without recti diastasis.
For the repair of a large hernia or hernia with recti diastasis please see: Abdominal Wall Reconstruction/Component Separation Repair.
A small incision is made just below/through the umbilicus (belly button) or over the epigastric hernia lump. The hernia is then dissected off the surrounding tissue including the belly button. It is then reduced (pushed back into the abdomen). If needed, a mesh is placed deep to the muscle layer.
The hernia defect is then closed with sutures and the incision is closed with sutures.
For the repair of a large hernia or hernia with recti diastasis please see: Abdominal Wall Reconstruction/Component Separation Repair.
A small incision is made just below/through the umbilicus (belly button) or over the epigastric hernia lump. The hernia is then dissected off the surrounding tissue including the belly button. It is then reduced (pushed back into the abdomen). If needed, a mesh is placed deep to the muscle layer.
The hernia defect is then closed with sutures and the incision is closed with sutures.

Cross section of abdominal wall.
Laparoscopic (keyhole surgery) procedures
Laparoscopic hernia repair
Three incisions are made on one side of the abdominal wall, away from the hernia site.
Gas is then introduced into the abdominal cavity, elevating the abdominal wall muscle away from the abdominal organs. The hernia content is identified (structures passing from the abdominal cavity to the abdominal wall and through the abdominal wall muscular defect). This is carefully pulled back into the abdominal cavity leaving the hernia defect exposed.
The hernia defect is then closed laparoscopically (from the inside). The hernia defect is then covered with mesh that is secured to overlying muscle with sutures and special clips (these dissolve by themselves).
The skin is then closed with dissolvable sutures.
Gas is then introduced into the abdominal cavity, elevating the abdominal wall muscle away from the abdominal organs. The hernia content is identified (structures passing from the abdominal cavity to the abdominal wall and through the abdominal wall muscular defect). This is carefully pulled back into the abdominal cavity leaving the hernia defect exposed.
The hernia defect is then closed laparoscopically (from the inside). The hernia defect is then covered with mesh that is secured to overlying muscle with sutures and special clips (these dissolve by themselves).
The skin is then closed with dissolvable sutures.
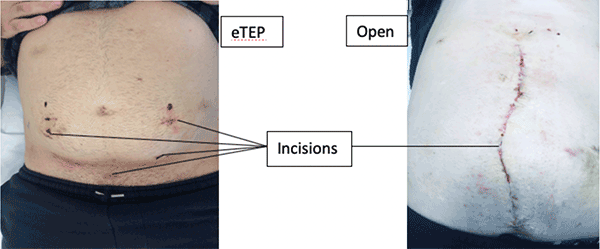
Extended Totally ExtraPeritoneal (eTEP) hernia repair
This is a minimal invasive method of repairing the hernia by placing a mesh in the retromuscular space. The use of this space enables the placement of a large size mesh.

This is achieved through typically 3–4 small incisions. Because of this, there is quicker recovery from the surgery compared to the open technique (where the operation was performed through a large midline incision).
Each approach has its own advantages and disadvantages, which will be discussed in detail at your consultation session.
At the Perth Hernia Institute, we believe that each hernia is unique and should be treated on an individual basis. We do not believe that all hernias should be treated with a single generalised approach. The treating surgeon should be able to discuss and offer all the surgical options to the hernia repair.
At the Perth Hernia Institute, we believe that each hernia is unique and should be treated on an individual basis. We do not believe that all hernias should be treated with a single generalised approach. The treating surgeon should be able to discuss and offer all the surgical options to the hernia repair.
Possible complications
Open umbilical/epigastric repair
Infection—this tends to occur around the belly button. This will require antibiotics.
Fluid collection (seroma) under the wound. In most patients, the body will reabsorb this. Occasionally an intervention may be needed.
Recurrence of the hernia. The use of mesh should reduce this rate to less than 2%.
Fluid collection (seroma) under the wound. In most patients, the body will reabsorb this. Occasionally an intervention may be needed.
Recurrence of the hernia. The use of mesh should reduce this rate to less than 2%.
Laparoscopic/eTEP repair
- Wound infection
- Mesh infection
- Wound haematoma/seroma
- Hernia recurrence
- Damage to abdominal organs. This may require an open major operative correction.
Postoperative care
Open umbilical/epigastric repair
The patient should expect to have some discomfort for one to two weeks. This can be alleviated with some oral pain relief.
The patient is encouraged to be active. (With restrictions of no heavy lifting for 4–6 weeks). However, caution is also advised when participating in exercise.
Please also see: Hernia – overview
The patient is encouraged to be active. (With restrictions of no heavy lifting for 4–6 weeks). However, caution is also advised when participating in exercise.
Please also see: Hernia – overview
Laparoscopic repair
The patient should expect to have some discomfort for one to two weeks. This can be alleviated with some oral pain relief, prescription given on discharge from hospital.
The patient is encouraged to be active. (With restrictions of no heavy lifting for 3 weeks). Caution is advised when participating in exercise.
The patient is typically reviewed 2–3 weeks after the operation.
Note: Patient will be given a post-operative management instruction sheet prior to the operation.
Please also see: Hernia – overview
The patient is encouraged to be active. (With restrictions of no heavy lifting for 3 weeks). Caution is advised when participating in exercise.
The patient is typically reviewed 2–3 weeks after the operation.
Note: Patient will be given a post-operative management instruction sheet prior to the operation.
Please also see: Hernia – overview
Clinical Associate Professor Hairul Ahmad
MB BS, FACEM (1999), FRACS, MS
Suite 12, Waikiki Specialist Centre,
217 Willmott Drive, Waikiki
Practice Details
Waikiki
Suite 12, Waikiki Specialist Centre,
217 Willmott Drive, Waikiki WA 6169
(08) 9592 2298
Fax: (08) 6314 1524
or email us
Office hours
9am–4pm Monday to Thursday
Affiliations




© 2024 All Rights Reserved. Content and images on this website are subject to copyright.
Email us | Sitemap | Disclaimer | Login